
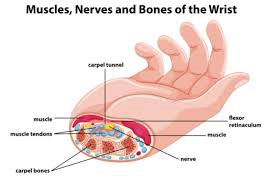
A nerve called Median nerve, which passes from the wrist supplies sensation to palm.
While passing through the wrist the nerve passes through a tunnel which is formed by bones and ligament. This tunnel becomes narrow and causes increased pressure on the nerve.
Due to the pressure the conduction is hampered causing symptoms.
Mechanical pressure on the wrist will cause symptoms and when you release the pressure the tingling will disappear.

It needs treatment ay early stage. If the median nerve is compressed for long period it will lead to atrophy of muscles of palm called ‘Muscles of Thenar eminence’.

At an early stage you would not be able to notice subtle wasting of muscle. However, a doctor, after examination, will be able to spot muscle wasting. Also, there will be weakness in strength of muscle on examination.
Conservative treatment in form of physiotherapy, ultrasound therapy, stretching exercises, anti-inflammatory.
Finding the underlying cause and its treatment can cause complete remission of symptoms.
The causes can be pathological requiring targeted treatment or physiological which often needs only symptomatic treatment and remits on its own.
The common causes are –
- Pregnancy
- Occupational – long hours of typing or computer related work
- Idiopathic – Middle aged female are more commonly susceptible without any definite underlying etiology.
- Imbalance in thyroid profile
- Local trauma
- Arthritis of wrist (either primary or secondary to rheumatoid arthritis, autoimmune conditions)
- Fractures and dislocations involving wrist. In these cases often needs surgical decompression in emergency.
- Diabetes Mellitus
- Obesity, Renal failure, tumours involving the wrist.
We use a standard questionnaire to find out the severity of the condition and then decide on surgery. The questionnaire is tested internationally and has proven benefits to rule out severity of disease and also to estimate the prognosis following surgery.
There are many methods of performing the surgery –
- Conventional open surgery – a incision given over the palm to release the retinaculum (a band covering the nerve which causes pressure over the nerve). There is a very good success rate. The surgery is usually done after infiltration of local anaesthesia. In special scenarios, general anaesthesia is given to perform the surgery
Usual duration of surgery – 30-40 min. - Endoscopic release – a small 1 cm incision is made and an endoscope is inserted to release the retinaculum. This technique is not routinely performed as there is still no evidence to prove its efficacy and safety over the conventional method
- Minimally Invasive – A small nick is made over wrist and scissors are passed percutaneously to cut the retinaculum percutaneously. This technique is not routinely performed as there is still no evidence to prove its efficacy and safety over the conventional method
This surgery is performed under local anaesthesia and hence very safe. Patient usually come in morning as out-patient and have the procedure done. After couple of hours of monitoring patients can go home with pain killer medications. No need of overnight stay.
Only single dose of antibiotic is needed during surgery. No post doses needed.
The first dressing change is usually done after a week to debulk the padding and apply a small dressing after that.
Sutures are usually removed at 10-14 days. However absorbable sutures are being used increasingly now-a-days to avoid hospital visit. Patent can themselves change dressing at home and the absorbable sutures just fall off after 2-3 weeks.
Usually the first visit is needed for suture removal if non absorbable sutures are used.
The second visit at 6 weeks and then at 16 weeks.
Physiotherapy is an essential and important aspect of therapy for carpal tunnel syndrome.
I usually provide my patients with post-operative physiotherapy care to teach them regarding the stretching exercises and strengthening exercises for better rehabilitation.
I advise my patients that they can return to work as per their pain tolerance usually after 2 weeks. They may need some adjustment in work conditions to avoid pressure locally to prevent scar irritation.
I usually advise my patients to avoid driving for 2 weeks till the sutures are removed and the pain is less. Usually patients have no pain after 2-3 weeks following surgery.