
There are 2 components in Hip replacement – The Ball ie. The Femur Head And the Socket ie. Acetabulum |
 |
Any lower limb surgery which reduces mobility for few days increases the risk of vein thrombosis. We take adequate precaution and prophylaxis for DVT.
Other risk factors include less than 1% risk of infection, change in limb length, risk of fracture while insertion of implant, risk of dislocation of joint, risk of implant loosening, nerve damage to sciatic nerve.
All the complications are treatable, and we advise all patients regarding adequate prevention and management of risk and complications.


What is DUAL MOBILITY CUP
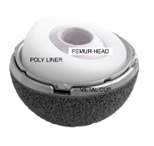
Improved range of movement with double surface of mobility. Less chance of dislocation.
HIGH POROUS COATED ACETABULUM CUP
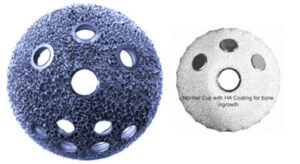
The surface of cup is coated with high porous coating which enhances scratch fit-fixation in bone, better bone ingrowth, less chance of implant loosening.
CONSTRAINED LINER FOR HIP DISLOCATION
A specially made liner to block the femur head within the cup. This is particularly helpful in patients with hip dislocation, old age, paraparesis or weak muscle tone, Parkinson’s disease, post hip fracture.